Overview
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
Causes
There are a number of factors that can increase the risk of an Achilles tendon rupture, which include the following. You?re most likely to rupture your Achilles tendon during sports that involve bursts of jumping, pivoting and running, such as football or tennis. Your Achilles tendon becomes less flexible and less able to absorb repeated stresses, for example of running, as you get older. Small tears can develop in the fibres of the tendon and it may eventually completely tear. There is a very small risk of an Achilles tendon rupture if you have Achilles tendinopathy (also called Achilles tendinitis). This is where your tendon breaks down, which causes pain and stiffness in your Achilles tendon, both when you exercise and afterwards. If you take quinolone antibiotics and corticosteroid medicines, it can increase your risk of an Achilles tendon injury, particularly if you take them together. The exact reasons for this aren't fully understood at present.
Symptoms
Patients present with acute posterior ankle/heel pain and may give a history of ?felt like someone kicked me from behind?. Patients may report a direct injury, or report the pain started with jumping or landing on a dorsiflexed foot. It is important to elicit in the history any recent steroid or flouroqunolone usage including local steroid injections, and also any history of endocrine disorders or systemic inflammatory conditions.
Diagnosis
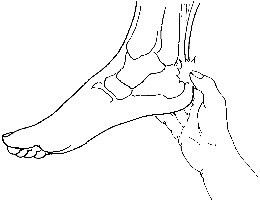
The diagnosis of an Achilles tendon rupture is made entirely on physical examination. Often, there is a substantial defect in the Achilles from 2-5 cm before it inserts into the heel bone. However, the main test is to determine whether the Achilles has been ruptured is the Thompson test. This essentially involves placing the patient on their stomach and squeezing the calf muscle. If the Achilles is intact, the foot will rise [plantar flex]. If it is ruptured, the foot will not move and will tend to be in a lower lying position.
Non Surgical Treatment
As debilitating as they can be, the good news is that minor to moderate Achilles tendon injuries should heal on their own. You just need to give them time. To speed the healing, you can try the following. Rest your leg. Avoid putting weight on your leg as best you can. You may need crutches. Ice your leg. To reduce pain and swelling, ice your injury for 20 to 30 minutes, every three to four hours for two to three days, or until the pain is gone. Compress your leg. Use an elastic bandage around the lower leg and ankle to keep down swelling. Elevate your leg. Prop you leg up on a pillow when you're sitting or lying down. Take anti-inflammatory painkillers. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil, Motrin) and naproxen (Aleve) will help with pain and swelling. However, these drugs have side effects, such as an increased risk of bleeding and ulcers. They should be used only occasionally unless your health care provider says otherwise and should be taken with food. Check with your doctor before taking these if you have any allergies, medical problems or take any other medication. Use a heel lift. Your health care provider may recommend that you wear an insert in your shoe while you recover. It will help protect your Achilles tendon from further stretching. Practice stretching and strengthening exercises as recommended by your health care provider. Usually, these techniques will do the trick. But in severe cases of Achilles tendon injury, you may need a cast for six to 10 weeks or even surgery to repair the tendon or remove excess tissue.

Surgical Treatment
The goal of surgery is to realign the two ends of the ruptured tendon to allow healing. There are multiple techniques to accomplish this goal that will vary from surgeon to surgeon. Recovery from this injury is usually very successful with return to full function in approximately 6 months. Post operatively casting is required with the use of crutches or other means to remain non-weightbearing for 4-8 weeks. This is followed by a course of physical therapy. Partial rupture may or may not require surgical intervention depending on the extent of injury but cast immobilization is a common requirement.
Prevention
The best treatment of Achilles tendonitis is prevention. Stretching the Achilles tendon before exercise, even at the start of the day, will help to maintain ankle flexibility. Problems with foot mechanics can also lead to Achilles tendonitis. This can often be treated with devices inserted into the shoes such as heel cups, arch supports, and custom orthotics.
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
Causes
There are a number of factors that can increase the risk of an Achilles tendon rupture, which include the following. You?re most likely to rupture your Achilles tendon during sports that involve bursts of jumping, pivoting and running, such as football or tennis. Your Achilles tendon becomes less flexible and less able to absorb repeated stresses, for example of running, as you get older. Small tears can develop in the fibres of the tendon and it may eventually completely tear. There is a very small risk of an Achilles tendon rupture if you have Achilles tendinopathy (also called Achilles tendinitis). This is where your tendon breaks down, which causes pain and stiffness in your Achilles tendon, both when you exercise and afterwards. If you take quinolone antibiotics and corticosteroid medicines, it can increase your risk of an Achilles tendon injury, particularly if you take them together. The exact reasons for this aren't fully understood at present.
Symptoms
Patients present with acute posterior ankle/heel pain and may give a history of ?felt like someone kicked me from behind?. Patients may report a direct injury, or report the pain started with jumping or landing on a dorsiflexed foot. It is important to elicit in the history any recent steroid or flouroqunolone usage including local steroid injections, and also any history of endocrine disorders or systemic inflammatory conditions.
Diagnosis
The diagnosis of an Achilles tendon rupture is made entirely on physical examination. Often, there is a substantial defect in the Achilles from 2-5 cm before it inserts into the heel bone. However, the main test is to determine whether the Achilles has been ruptured is the Thompson test. This essentially involves placing the patient on their stomach and squeezing the calf muscle. If the Achilles is intact, the foot will rise [plantar flex]. If it is ruptured, the foot will not move and will tend to be in a lower lying position.
Non Surgical Treatment
As debilitating as they can be, the good news is that minor to moderate Achilles tendon injuries should heal on their own. You just need to give them time. To speed the healing, you can try the following. Rest your leg. Avoid putting weight on your leg as best you can. You may need crutches. Ice your leg. To reduce pain and swelling, ice your injury for 20 to 30 minutes, every three to four hours for two to three days, or until the pain is gone. Compress your leg. Use an elastic bandage around the lower leg and ankle to keep down swelling. Elevate your leg. Prop you leg up on a pillow when you're sitting or lying down. Take anti-inflammatory painkillers. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil, Motrin) and naproxen (Aleve) will help with pain and swelling. However, these drugs have side effects, such as an increased risk of bleeding and ulcers. They should be used only occasionally unless your health care provider says otherwise and should be taken with food. Check with your doctor before taking these if you have any allergies, medical problems or take any other medication. Use a heel lift. Your health care provider may recommend that you wear an insert in your shoe while you recover. It will help protect your Achilles tendon from further stretching. Practice stretching and strengthening exercises as recommended by your health care provider. Usually, these techniques will do the trick. But in severe cases of Achilles tendon injury, you may need a cast for six to 10 weeks or even surgery to repair the tendon or remove excess tissue.
Surgical Treatment
The goal of surgery is to realign the two ends of the ruptured tendon to allow healing. There are multiple techniques to accomplish this goal that will vary from surgeon to surgeon. Recovery from this injury is usually very successful with return to full function in approximately 6 months. Post operatively casting is required with the use of crutches or other means to remain non-weightbearing for 4-8 weeks. This is followed by a course of physical therapy. Partial rupture may or may not require surgical intervention depending on the extent of injury but cast immobilization is a common requirement.
Prevention
The best treatment of Achilles tendonitis is prevention. Stretching the Achilles tendon before exercise, even at the start of the day, will help to maintain ankle flexibility. Problems with foot mechanics can also lead to Achilles tendonitis. This can often be treated with devices inserted into the shoes such as heel cups, arch supports, and custom orthotics.
 RSS Feed
RSS Feed